
Osteoarthritis of the knee is a degenerative form of arthritis. When a joint develops osteoarthritis some of the cartilage covering the joint surfaces gradually wears away. It occurs most often in people 50 years of age and older but can occur in younger age groups as well. Osteoarthritic changes in the joint are partly the result of the inflammatory process and partly your body`s attempt to repair the affected area.
What causes knee osteoarthritis?
There are many factors that can increase the risk of osteoarthritis:
- Age - Knee osteoarthritis usually starts from the late 40s onwards. We don’t fully understand why it is more common in ageing individuals. However research indicates that as people age their muscles weaken and may contribute to the osteoarthritic process.
- Gender - Knee osteoarthritis is twice as common in women as in men. Researchers believe that female hormones have an effect on the cartilage that sits between and cushions the bones. After the menopause women’s hormone levels can reduce, which means they lose the protection on the cartilage, and the risk of developing changes in the knee joint is increased.
- Being overweight - Research shows that individuals who are classified as ‘obese’ are up to four times as likely to develop knee osteoarthritis. Body Mass Index (BMI) is how the relationship between your weight and height is calculated and deemed to be normal or abnormal. Being overweight can increase the load on the joint, which in turn can speed up the wear in the cartilage, increasing the risk of developing osteoarthritis.
- Joint injury - Normal movement and exercise don’t cause knee osteoarthritis. However, very hard and repetitive activities or physical jobs can increase the risk. High intensity activities such as kneeling when at work can lead to joint injury.
- Genetic – The genes inherited from your parents can play a role in osteoarthritis of the knee. If you have a parent, brother or sister with knee osteoarthritis you will have a higher chance of developing it yourself. However some researchers claim this is due to factors that families tend to share such as dietary intake, physical activity levels and occupations.
What are the symptoms of osteoarthritis in the knee?
The main symptoms of osteoarthritis of the knee are:
- Pain: worse with movement, better with rest.
- Stiffness: worse in mornings after period of rest
- Restricted range of movement: can feel/sound like it crunches/creaks
- Giving way of knee
- Swelling
- Loss of muscle bulk at front of thigh
Are there any surgical options for knee osteoarthritis?
If your symptoms of pain and reduced ROM are significantly disabling then total knee joint replacement is the surgical treatment of choice. This involves removing the affected bone of the knee joint and replacing it with a “prosthesis” or “artificial joint” made from metal and plastic. This new joint prevents the bones from rubbing together and provides a smooth knee joint.
The focus of knee joint replacement is pain relief. Be aware there are complications in approx. 10% of patients. Indications for surgery are high levels of pain despite conservative care, difficulty sleeping due to pain and reduced levels of function secondary to pain. It is important to note that a significant amount of physiotherapy and exercise are required to achieve best results in regard to function and range of movement post-surgery.
See our section on knee joint replacement for more details.
What can you expect from a total knee replacement?
- Pain Relief in about 90% of cases
- Restored function and mobility
A total knee joint replacement will allow you to carry out normal activities of daily living. It may or may not allow you to return to active sports or heavy labour. However if you take part in high impact activities and are overweight, this may speed up the wear and tear process and could result in the artificial knee loosening or becoming painful.
Correction of deformity
Often with severe arthritis of the knee you can have ‘bow legs’. During surgery your surgeon will try and correct this deformity for you.
Are there any potential complications from undergoing a total knee replacement?
There are potential complications involved in having a total knee joint replacement which are as follows:
- Infection: Occurs in less than 2% of patients.
- Major medical complications such as heart attack or stroke.
- Chronic illness may increase the potential for complications.
- Wound infection.
- A foot drop: this is where the muscles that help move your ankle become permanently weak or not working at all. This is due to nerve damage and may or may not fully recover.
- Difference in leg length.
- Deep Vein Thrombosis (DVT) which is a blood clot in your leg. Symptoms of this include calf pain/tightness, calf throbbing, lower limb swelling which is new or increasing, redness or inflammation to your calf or thigh or calf feeling hot.
- Pulmonary Embolism (PE): Blood clot formed in your leg breaks out and travels to your lung. Risks of this being life threatening is low.
What can I do for my knee osteoarthritis?
There is no cure for osteoarthritis, but there is a lot that you can do to improve your symptoms. Self-help or self-management is very important to relieve the pain, stiffness and reduce the chances of your arthritis becoming worse. The one professional who can best manage your symptoms is you!
Osteoarthritis exercises
The exercises in the videos below have been provided to help with your knee pain. If there is any doubt about your fitness to do these exercises then please discuss this with your GP.
You may find that these exercises may slightly increase your symptoms initially. However you should find that the exercises themselves will become easier to do and that you begin to move your knee more easily. It can take around 12 weeks for you to notice a great improvement.
If the exercises do cause some discomfort, then taking prescribed medication from your GP or pharmacist may help you to continue to exercise.
If these exercises cause a large increase in your pain, or after 12 weeks there are no noticeable changes in your day to day symptoms, please contact your GP or NHS Inform for more advice.
The guide below will help ensure you are working at the right level.
Pain during exercise
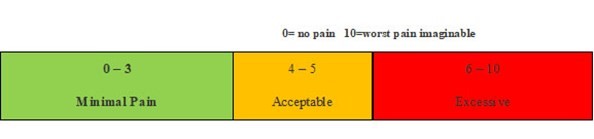
Within the scale, aim to stay in the green or amber boxes. If you are in the red area then you can modify the exercises by:
- reducing the amount of movement during an exercise
- reducing the number of repetitions
- reducing the weights
- reducing your speed
- increasing rest time between sets
Pain after exercise
Your pain or other symptoms should return to your pre-exercise baseline within 30 minutes of exercising. On the morning after your exercises, you should not feel an increase in pain or stiffness that lasts longer than 60 minutes.
Disclaimer
Please note: These exercises should not be used without prior consultation with a medical professional as the use of the wrong exercise may cause additional health related issues and discomfort. NHS Ayrshire & Arran and MSK NHS Ayrshire & Arran are not liable or responsible for any harm, losses or damages whatsoever resulting from the use or misuse of the information contained in or implied by the provided information in each video. These are provided for information only.
If you have any concerns about your ability to perform exercise then please discuss your concerns with your doctor or healthcare provider prior to participating in any advice that is on the MSK NHS Ayrshire & Arran website.
It is recommended to use your ice pack (cryocuff) or cool pack after your exercises to reduce the pain and discomfort this may cause.
Please choose the most relevant exercise section for you.
Section 1: Stretching
Exercise 1: Quadriceps stretch
The quadriceps stretch aims to improve the flexibility of the muscles at the front of your thigh which attach from the hip to the knee. Hold the stretch for a slow 30 second count and repeat five times.
Exercise 2: Hamstring wall stretch
The hamstring stretch aims to improve the flexibility of the muscles at the back of your thigh which run roughly from your bottom to just below your knee. Hold the stretch for a slow 30 second count and repeat five times.
Exercise 3: Gastrocnuemius/Soleus stretch
This exercise focuses on stretching the muscles of the lower leg commonly known as the ‘calf’ muscles (the gastrocnemius and soleus). Hold each stretch for a slow 30 second count and repeat five times.
Exercise 4: Adductor stretch
The adductor stretch aims to stretch a group of muscles along the inner thigh, commonly called the groin muscles. Hold the stretch for a slow 30 second count and repeat five times.
Section 2: Strengthening
Exercise 1: Wall squats
The wall squat is a strengthening exercise for several muscles in the lower body that need to be strong to assist with your symptoms. This exercise works the gluteus maximus (or bottom muscles), the hamstrings (the muscles of the back of your thigh), the quadriceps (the muscles down the front of your thigh) and the core muscles (the muscles of your abdomen). Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 2: Forward step-up
The forward step-up is a strengthening exercise which targets the quadriceps (the muscles down the front of your thigh), the gluteus maximus (bottom muscles or glutes), the hamstrings (the muscles of the back of your thigh) and the core muscles (the muscles of your abdomen). Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 3: Heel drop
The heel drop exercise is used to improve the strength of the gluteus maximus (bottom muscles or glutes), the quadriceps (the muscles down the front of your thigh), and the hamstrings (the muscles of the back of your thigh) and to improve your lower body control and balance. Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 4: Mini squat
If you do not feel confident with the heel drop exercise (exercise 6) then an alternative exercise that can be done without a step is the mini squat. This focuses on strengthening the gluteus maximus (bottom muscles or glutes), the hamstrings (the muscles of the back of your thigh), the quadriceps (the muscles down the front of your thigh) and the core muscles (the muscles of your abdomen). Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 5: Pelvic drops
The pelvic drop exercise is used to strengthen the gluteus medius muscle (the muscle at the side of your bottom). Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 6: Bridging
This exercise is a very effective way of strengthening multiple muscle groups of the lower back and legs. Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 7: Sit-to-stand
The sit-to-stand strengthening exercise primarily targets the gluteus maximus (bottom muscles or glutes), the hamstrings (the muscles of the back of your thigh), the quadriceps (the muscles down the front of your thigh) and your back muscles. Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.
Exercise 8: Alternating lunges
Lunges are lower body strengthening exercises that work several muscle groups at once. The targeted muscles groups include the gluteus maximus (bottom muscles or glutes), the hamstrings (the muscles of the back of your thigh), the quadriceps (the muscles down the front of your thigh) and your back muscles. Start at one set of 15 repetitions daily and slowly increase this to three sets of 15 repetitions as you become stronger and fitter.