
We have taken a unique and proactive approach to the care, recovery and rehabilitation of our joint replacement patients. You and the various health care professionals will share the responsibility for your care.
Rapid recovery is a patient-focused experience, which starts with the decision to operate, to when you are recovering at home. This shared responsibility for treatment, recovery and rehabilitation is fundamental to the success of your operation. The programme provides the knowledge and skills to allow you to do this and will also develop your independence.
This webpage has been designed by the orthopaedic team to provide you, your family and your friends with information about your knee replacement and what to expect before, during and after your stay in hospital.
This advice will help you prepare for surgery, recovery and rehabilitation. You should read this page thoroughly before your surgery and write down any questions you may have.
Understanding arthritis and knee replacement
Joint deterioration can affect every aspect of a person’s life. In its early stages, it is common for people to ignore the symptoms of osteoarthritis. However, as the condition progresses, activities such as walking, driving and standing, can be painful and very difficult. This guide will help you understand some of the basics of anatomy, arthritis and knee replacement surgery. It is for information only and is not intended to replace the expert guidance of your orthopaedic surgeon. If you have any questions or concerns, you should speak to your orthopaedic surgeon or any member of your care team.
The first knee replacement procedure was performed more than 30 years ago. Since then, millions of people have had knee replacements. Knee replacement surgery is a fairly routine procedure and is usually an extremely successful surgical procedure. You may think that the term ‘replacement’ means that the surgeon removes the entire knee. However, your surgeon only ‘re-surfaces’ the damaged cartilage found at the ends of the bones in your joint.
The knee
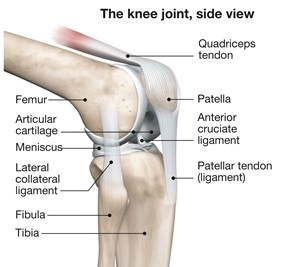
The knee is a hinge joint formed by the tibia (shinbone), femur (thighbone) and patella (kneecap). The ends of the bones in the joint are covered with cartilage a tough lubricating tissue that helps cushion the bones during movement. Arthritis is a condition that affects joint cartilage and it develops over years of constant motion and pressure in the joints. As the cartilage continues to wear away, the joint becomes increasing painful and difficult to move. There are over 100 different kinds of arthritic conditions that can affect the human body and there are millions of people who are affected with arthritis each year.
Osteoarthritis
Osteoarthritis, often referred to as OA, is the most common form of arthritis, and is the most common reason for joint replacement surgery. Osteoarthritis is a degenerative condition that destroys the joint cartilage, often leading to painful narrowing of the knee joint. It can cause pain, stiffness, swelling and loss of motion in the joint, which may vary in duration and severity from person to person.
Treatments such as the relief of pain, physiotherapy exercise and losing weight, can help control the symptoms of osteoarthritis for a time. When these treatments no longer provide adequate relief from pain, your surgeon may recommend a total joint replacement. Your surgeon will have assessed your individual condition and prescribed a treatment that will give you the best results.
Types of knee replacements
Total knee replacement
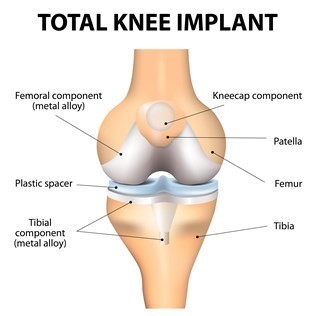
Total knee replacement involves removing the diseased cartilage and resurfacing it with orthopaedic implants. During surgery, the joint is exposed by an incision made down the centre or off to the side of the knee. The damaged bone ends are then resurfaced with components implanted with bone cement. These components are designed to re-create the natural contours of the bones in a healthy knee. The metal and polyethylene (plastic) implants allow the bones to glide smoothly against each other like natural cartilage.
Partial knee replacement
A partial knee is intended for use in individuals with osteoarthritis limited to the inner compartment of the knee.
Partial knee replacement involves removing the cartilage and a small amount of bone in the compartment of the joint and resurfacing it with orthopaedic implants. Unlike a total knee replacement, the good cartilage on the opposite side of the knee and the ligaments which cross within the knee are retained. This means that you will have more normal function and movement of your knee following surgery and will be able to return to excellent levels of activity.
If, during surgery, your surgeon encounters reasons why your knee is not suitable for a partial knee replacement, then, in most cases, a total knee replacement will be done.
Surgery will take approximately one hour but you will be taken to the recovery room before returning to your room.
Revision knee replacement
Much of the information on this webpage, such as the preparation for surgery advice and exercise information, will apply to those patients who are undergoing primary surgery. However, due to the complexities of revision surgery it is important to discuss the preparation and rehabilitation advice for this surgery. You should not expect to recover and rehabilitate at the same pace as those patients undergoing primary total knee replacement.
Revision total knee replacement is an effective treatment for the relief of pain from infection or loosening of a knee replacement. The revision knee replacement involves removing the old knee replacement and replacing it with a new one. The operation can take up to four to five hours to complete. Infection or loosening are the two main reasons why a knee replacement may need to be re-done.
Infection in revision knee
- First stage: The joint is removed in theatre, and left out for a period of between six weeks and three months until antibiotic therapy is completed – you may not need to stay in hospital for this period of time.
- Second stage: Once the surgeon is satisfied the infection is treated, a new joint will be put in.
Loosening of the joint replacement
Your old knee replacement will be removed in theatre and, providing there are no signs of infection, a new knee will be put in at the same time.
If there is an infection, the surgeon will need to leave the joint out. Sometimes infection only becomes apparent during surgery. In this case, the surgeon will remove the knee replacement and treat you with antibiotics as for the first stage.
Bone grafting
This may be required when the joint is replaced. This is usually the case in more complex procedures. The bone graft may come from previous patients and will have been subjected to a rigorous screening process, similar to blood for transfusion.
If you have a bone graft you will need to protect it for several weeks until x-rays show that it is strong enough to take your weight. Your surgeon will guide this process, and the team will keep you informed.
Walking again after revision of knee replacement
Your consultant or physiotherapist will let you know if your knee needs to be:
- non-weight bearing – You can only walk using crutches or a walking frame. You should not stand on your operated leg at all.
- touch-weight bearing – You are able to put your foot to the floor but with very little weight through it.
- partial-weight bearing – You are able to put around half of your weight through your leg.
- fully-weight bearing – Using sticks, you are able to put all your weight through your revised joint.
What can I expect from a total knee replacement?
- Pain relief - A total knee replacement will provide relief from knee pain in 90 per cent of patients.
- Restored function and mobility – A total knee replacement will allow you to carry out normal activities of daily living. The artificial knee may or may not allow you to return to active sports or heavy labour. Your consultant will advise you. If you take part in high impact activities and are overweight, this may speed up the wear and tear process and could result in the artificial knee loosening or becoming painful.
- Correction of deformity - Often with severe wear and tear of the knee you can have ‘bow legs’. During surgery your surgeon will try and correct this deformity for you.
Total knee replacement or knee surgery is an elective operation, which means it is not a matter of life or death. The decision to have the operation is not made by the doctor; it is made by you. It is you who must weigh up the risks and benefits for you and be sure you can accept the risks.
The real success of your knee replacement depends partly on you – your motivation, positive attitude, commitment to exercising and knowing your limitations for a specified period of time after the surgery.
Complications
Although it is rare, complications can occur during and after surgery. Total knee replacement is 90 per cent successful. However, ten per cent of patients can develop complications.
Serious complications, such as knee joint infection, occur in less than two per cent of patients. Major medical complications, such as heart attack or stroke, occur even less frequently. Chronic illness may increase the potential for complication. Though uncommon, when these complications occur, they may prolong or limit your full recovery.
Although implant surgery is extremely successful in most cases, some patients still experience pain and stiffness. Most patients, however, feel that the relief from the arthritic pain is so good that a certain amount of stiffness does not bother them.
No implant will last forever and factors such as your post-surgical activities and weight can affect the life of the implant. Make sure you discuss all of the risks with your surgeon so that you can minimise the potential for complications.
Wound infection
There is a small risk that the wound on your knee can become inflamed, painful and weep fluid, which may be caused by infection.
It is common for the wound to have some leakage – this fluid is clear and non-smelling. If you, your community nurse or GP think you have an infection you should use the contact details given to you on discharge from the ward.
Your surgeon will want to know about any concerns regarding your wound. The majority of wound infections can be treated by a course of antibiotics and often settle down following treatment. Deep wound infection where the new knee is infected may mean that you need revision surgery in two stages. The leg can be weak and you would need to use a stick or crutch when walking.
You can help prevent infections in the wound firstly, by ensuring you are thoroughly showered and clean prior to your surgery. After your surgery you must keep the incision area clean and dry. In the long term, you should check with your doctor and dentist prior to any dental treatment or if you have a skin or urine infection as you may need antibiotics. The risk of developing an infection following a knee replacement is one to two per cent.
Methicillin resistant staphylococcus aureus (MRSA)
Micro-organisms, or germs or bacteria, are all around us. We all carry millions of them both on the inside and outside of our bodies. We can only see them with a microscope. They generally do us no harm. Most bacteria protect us from infections, but some can cause infections.
Methicillin resistant staphylococcus aureus, or MRSA is a bacterium that can no longer be treated by some commonly used antibiotics. MRSA can survive on the body causing you no problems. However, if it gets into a wound, it can prove more difficult to treat than some other infections.
Outside the healthcare setting MRSA is not a problem. However, in hospital, there are patients with wounds and sick people who are more susceptible to infections. This is why we may place you in a side room or on an alternative ward during your stay to prevent the spread of MRSA.
The staff will not treat you any differently but will wear apron and gloves when caring for you. If they come in to talk to you or deliver your meals, no precautions are necessary.
However, they will need to wash their hands before entering and leaving your room. MRSA will not interfere with any care you require, all staff will know the precautions they need to take.
Visitors do not need to wear gloves and aprons but must wash and dry their hands thoroughly on entering or leaving the room, and any cuts should be covered. If they are visiting another patient, they should see you last if you have MRSA.
MRSA will not affect your discharge home and you are no more likely to get an infection than anyone else.
Foot drop
This occurs when the nerves that control the muscles in the foot become stretched or damaged as a complication of your surgery leaving you with a weakened or dropped foot. This complication is rare, but can happen in one in 1000 patients.
Difference in leg length
Your consultant will aim to give you equal leg length. However if arthritis or wear and tear has destroyed some of your bone this is not always possible and may cause your operated leg to become slightly shorter. This is less likely with a knee replacement than a hip replacement. However, if this does occur, you may need to wear a raised shoe or insole.
Loosening of the prosthesis
After 15 years, around a quarter of all artificial knees will appear loose on x-ray. Less than half of these (five to ten per cent) will become painful and will need an operation to replace the worn artificial knee. Loose or painful artificial knees can usually, but not always, be replaced.
Deep vein thrombosis (DVT)
There is a ten to 20% risk of developing a deep vein thrombosis (DVT) following surgery. This is the term used when a blood clot develops in the deep veins of your leg, most frequently below the knee. When you are first seen at preadmission, we will assess you for the risk of DVT. Your treatment in prevention of clots may vary according to your risk factors – for example, any previous history of DVT or the type of surgery you are having.
If you stay in bed for any period of time, the blood flow to your legs will slow down. This is because your leg muscles are not squeezing the veins as they normally do when you walk. Sometimes, the blood flow can get so slow that a clot is able to form.
The main causes of DVT are lying or sitting with no movement, and clotting changes within the blood vessels – blood naturally tries to clot to mend the damaged vessels.
The signs and symptoms are:
- Calf pain or tightness
- Calf throbbing
- Lower limb swelling that is new or increasing
- Redness or inflammation to your calf or thigh area
- The calf feels hot
Pulmonary embolism (PE)
This can happen when a part of a blood clot formed in your leg vein breaks off and travels to your lung. The risk of developing a life threatening pulmonary embolism is low.
The signs and symptoms are:
- difficulty in breathing
- chest pain or discomfort
- bluish tinge to lips, face or extremities
- coughing with blood-stained phlegm
- sudden collapse
Treatment is the same as DVT, but requires a longer hospital stay.
Measures to prevent deep vein thrombosis and subsequent pulmonary embolism include:
- Blood thinning drugs – You may be given drugs to thin the blood and make it less likely to clot.
- An injection administered just below the skin surface into the skin fold of the abdomen. Generally this will start on the day of surgery and continue everyday until two weeks after your operation.
- Prescribed tablets to take during your stay and on discharge home, to continue for two weeks after your operation.
To reduce the risk of clots:
- Get up and mobilise yourself as soon as you are advised after surgery.
- Do your exercises independently, once we have advised it is safe to do so.
- Do your breathing exercises and foot and ankle exercises.
- Take your medication as prescribed.
- If you smoke, once you have decided to go ahead with surgery, you should stop smoking.
Due to the possible increased risk of a blood clot or embolus, we advise that you do not fly six weeks pre or six weeks post surgery. If you are flying long haul, then please inform your surgeon’s secretary.
Preparing for surgery
You will be given an appointment to attend for pre-operative assessment clinic. This can last two to three hours and helps your anaesthetist consider any medical problems which may affect your risks and complications during the anaesthetic and/or surgery. You will be given time to ask any questions you have and are welcome to bring a friend or relative with you.
During this appointment you will be asked about the following:
- General health and wellbeing including what level of exercise you are able to do.
- Previous medical history including any anaesthetics you may have had. This includes any family history of anaesthetic complications.
- Allergies, smoking status, alcohol intake.
- Medication history – please bring all your medicines with you to this appointment. You will be advised of any medication you need to stop prior to your operation.
You will have some investigations carried out such as heart trace (ECG), blood tests and swabs to check for MRSA.
One of the blood tests is to identify if your blood count is low. If so, you may need to take iron tablets prior to your operation. This helps reduce the risk of the potential need for a blood transfusion afterwards.
Health and wellbeing lifestyle changes
It is important to be as fit as possible before undergoing joint replacement surgery. Taking part in a physiotherapist-prescribed exercise program before surgery can make a more rapid recovery.
Moderate exercise is an integral part of treating arthritis. Low-impact exercise will not wear out your joints. Although exercise may sometimes cause discomfort, proper exercise will help nourish the cartilage, strengthen the muscles, and prolong the life of your joints. Always follow your surgeon’s instructions and never do any exercises without first speaking with your surgeon or physiotherapist.
Your surgeon or physiotherapist can give you an individual programme.
- Make a plan. Write it down. Set realistic goals.
- Exercise at the same time each day so it becomes part of your routine.
- Look for an appropriate exercise class.
- Stay in the habit of doing some exercise each day.
- Vary your exercise routine and rotate your exercises.
- Evaluate your progress and enjoy your success.
- Stop when you get tired.
The UK Chief Medical Officers’ Guidelines recommend each week adults do:
- At least 150 minutes moderate intensity activity, 75 minutes’ vigorous activity, or a mixture of both
- Strengthening activities on two days
- Reducing extended periods of sitting
Swimming is an excellent form of exercise to help manage arthritis pain. Water’s buoyancy helps protect your joints from impact injury. Water also resists movement, which is helpful for building strength. Water pressure can also assist with reducing the swelling in joints and oedema in the legs.
Walking is an excellent form of endurance exercise for almost anyone, including those with arthritis. Be sure to have a good pair of walking shoes to help cushion impact.
Regular cycling or using a static exercise bike is an excellent endurance exercise. However, this may exacerbate patients suffering with knee problems, so always discuss this option with your consultant. Be careful not to increase the resistance or ride up and down hills too quickly.
If you smoke, it is essential you stop smoking before you have any surgery. It is necessary to stop smoking at least two to four weeks before the planned procedure. Smoking impairs the transfer of oxygen to the healing tissues, which may increase healing time and the possibility of other complications.
It is important to disclose your weekly alcohol intake when asked. Patients that suddenly stop their regular alcohol intake can experience withdrawal. This can be very unpleasant and dangerous. If the medical staff are aware of this prior to surgery, medication can be prescribed to minimize the symptoms.
Good nutrition is important before joint replacement surgery. If you are overweight, it is very important to reduce your weight in preparation for your surgery. This will help to reduce any risks associated with the anaesthetic and ensure you get the maximum benefit from your surgery.
If you have diabetes, it is also important to ensure that your blood sugars are well controlled prior to surgery.
If you have any concerns about your diet, discuss them with your doctor and you can be referred to a dietitian if required.
Things to do before your operation
Medications
Make sure you tell the doctor, nurse or hospital pharmacist everything that you are taking, including any creams, inhalers, eye drops, herbal supplements, and homoeopathic medicines and over the counter medicines.
Take all of your medicines, even natural remedies, in their original containers, when you attend your pre-operative assessment. The pharmacist will then be able to tell you if you need to stop taking any of your medications, and when. This is important because a number of drugs and herbal remedies may increase the risk of bleeding or blood clots or may interact with your anaesthetic and potentially cause complications.
If you do not let us know about all your medication, your operation could be postponed.
Ensure you have an adequate supply of your regular medicines for when you are discharged, as we can only supply new medicines when you are discharged.
Prepare your home
Remember, when you first go home you will not be fully mobile and may have some restrictions on what you are able to do.
Think about the things you normally do and make some adaptations. For instance, if you keep your mugs or plates in a low cupboard, consider moving them to a more accessible place for a short while after your operation. If you have to cook for yourself, consider making or buying some ready meals that are easy to prepare when you come home. It is also wise to be up to date with household chores like cleaning and laundry. You will not be able to do these in the first few weeks after your operation. Involve your ‘coach’ in making the necessary preparations.
Pre-operative education
This can take place in many forms. You may be given written/verbal or face to face information. The aim of this is to ensure you are clear in your expectations of surgery short and long term.
Your team
This hospital is committed to providing the best care as well as a positive healthcare experience for you and your family. Your care team is made up of many dedicated professionals who will work with you to make your stay at our hospital pleasant and your transition back to home as smooth as possible.
Your orthopaedic surgeon works with a network of orthopaedic specialists. These people work together to treat you as an individual providing the best care available for a wide range of medical concerns, from pre-diagnosis through treatment and on to therapy and rehabilitation.
Our ultimate goal is to help you regain your ability to engage in life at the level that gives you the greatest satisfaction.
Anesthetic
There are various different types of anesthetic and your anaesthetist will explain the different types available to you.
There are also different methods of providing pain relief (analgesia) for the first few days following your surgery.
During any form of anesthesia, it is standard practice to insert a tiny plastic tube (cannula) into one of the veins of your arm and to attach a small clip to one of your fingers to monitor the levels of oxygen in your blood. You will also have a heart trace, or electrocardiogram (ECG) and we will monitor your blood pressure. We may also give you fluids through the plastic cannula during and after the operation.
There are two major options for your anesthetic: a spinal anesthetic or a general anesthetic.
Spinal anesthetic
This type of anesthetic means you will be numb from the waist down and feel no pain during the operation. You can also be asleep if you wish. This is different from a general anesthetic, where you are unconscious with a breathing tube.
During a spinal anesthetic:
- We will inject you with a local anesthetic near to the nerves in your lower back. This can be given with you sitting up or lying on your side.
- You are numb from the waist downwards.
- You will feel no pain, but you remain conscious.
- You can also have drugs which make you feel sleepy and relaxed (sedation) or you can be completely asleep.
- Depending on the medication used it can take anywhere between two and six hours before normal movement in your legs return.
- A long-acting pain-relieving medicine may be injected along with the local anesthetic. This can give pain relief for up to 24 hours.
- Your anesthetist will ask you to keep quite still while the injection is given.
- You may notice a warm tingling feeling as the anesthetic begins to take effect.
- In around 10 minutes your legs will go completely numb and you will not be able to move them, this is normal.
- Your operation will only go ahead when you and your anesthetist are sure that the area is numb.
- If you are not having sedation, you will remain alert and aware of your surroundings. A screen shields the operating site, so you will not see the operation unless you want to. Some people take headphones and listen to music during surgery.
- Your anesthetist is always near to you and you can speak to them whenever you want to.
Advantages of spinal anesthetic are as follows:
- You should have less sickness and drowsiness after the operation and may be able to eat and drink sooner.
- You will be able to sit out of bed and take some supervised steps on the same day as your operation. This helps to avoid blood clots in the legs and lungs.
- There may be less bleeding during surgery and you will be less likely to need a blood transfusion.
- You remain in full control of your breathing and you will breathe better in the first few hours after the operation. This reduces the risk of chest infection.
- You do not need so much strong pain relieving medicine in the first few hours after the operation.
Because of the advantages spinal anesthetic gives, it is the most common type of anesthetic for knee replacement surgery. We recommend this type of anesthesia for your operation.
General anesthetic
A general anesthetic is when you are given drugs to make sure you are unconscious. During this time, you will feel nothing.
During a general anesthetic, you will receive:
- Anesthetic drugs – an injection or a gas to breathe.
- Strong pain relief drugs – morphine or something similar.
- Oxygen to breathe.
- In some cases, you may need a drug to relax your muscles.
- You will need a breathing tube in your throat to make sure that oxygen and anesthetic gases can move easily into your lungs. If you have been given drugs that relax your muscles, you will not be able to breath for yourself and a breathing machine (ventilator) will be used.
- When the operation is finished the anesthetic is stopped and you regain consciousness.
Advantages of general anesthetic:
- You will be unconscious during the operation.
Disadvantages:
- A general anesthetic alone does not provide pain relief after the operation. You will need strong pain relieving medicines afterwards, which make some people, feel quite unwell and sick.
- Some patients may feel sick, nauseous, light headed or drowsy after their operation. Some patients may also be mildly confused for a few days. This may prevent you from sitting out of bed soon after surgery and delay your mobilisation.
Regional analgesia
Regional analgesia is when we give pain relief to make an area of the body numb. This is carried out in addition to an anesthetic (spinal or general). The pain relief provided by regional analgesia means you will need less or no strong pain relieving drugs like morphine after your operation. There are several techniques that can be used.
1 – Nerve block
This is an injection of local anesthetic near to the nerves which go to your leg. It is used in combination with a spinal or general anesthetic. Part of your leg should be numb and pain-free for many hours after the operation, and you may also not have full strength in your leg during this time. The pain relief can be extended for a few of days by pumping a local anesthetic solution into a very fine tube left next to the nerve in your leg.
If you are having a general anaesthetic, this injection may be done before the anaesthetic starts, or it may be done when you are unconscious. Either way, it is a simple procedure.
A nerve block gives good pain relief for several days. It is less painful when bending your knee in the first few days, and less morphine is needed for pain relief. As only one leg is numb, it is easier to walk. However, a temporary weakness in the leg can make walking more difficult initially.
2 – Epidural analgesia
This is similar to a spinal anesthetic, but is used to provide pain relief after the operation. A small plastic tube, known as an epidural catheter, is passed through a needle into a place near to the nerves in your back. You receive local anesthetics and pain relief drugs through this tube, relieving pain and reducing all feeling in your lower body. This effect can be made to last several days.
If you are having a general anesthetic, this injection may be done before the anesthetic starts, or it may be done when you are unconscious. Either way, it is a simple procedure. An epidural can also be used in combination with a spinal anesthetic.
An epidural has all the advantages of the spinal anesthetic and gives good pain relief for several days. It is less painful when bending your knee in the first few days, and you will need less morphine for pain relief.
However, you are more likely to need a catheter in your bladder, as the epidural may make it difficult to pass urine. You may find that there is a delay in starting walking after your operation – usually no more than a day – due to numbness and weakness in your legs.
Side effects, complications and risks of anaesthesia
Serious problems are uncommon but there is still a small risk. Modern equipment, training and drugs have made anaesthesia a much safer procedure in recent years. Anaesthetists take a lot of care to avoid all the risks described in this booklet. Your anaesthetist will be happy to give you more information about any of these risks and the precautions taken to avoid them.
Common and very common side effects
- You may have pain around injection sites.
- You may have pain and you may have received strong pain relieving drugs.
- You may not be able to pass urine or you may wet the bed. This is because you are lying down.
- A soft plastic tube may be put in your bladder (a catheter) to drain away the urine for a day or two. This is more common after spinal or epidural anaesthetics.
- With spinal, epidural or nerve block, you will not be able to move your legs properly for a while. If pain relieving drugs are given in your spinal or epidural as well as local anaesthetic, you may feel itchy. You may also get a severe headache lasting a few days.
- With general anaesthetic, you may feel sick or have a sore throat. This can be treated with anti-sickness drugs and painkillers. You may feel drowsy, have a headache, shivering or blurred vision. This can be treated with fluids or drugs. You may even have difficulty breathing – this usually improves rapidly. Confusion and memory loss are common in older people, but are usually temporary.
Uncommon side effects and complications
- There is a very small risk of heart attack or stroke.
- If you have had a general anaesthetic, there is a small risk of damage to teeth, lips and gums, chest infection and awareness – that is becoming conscious during a general anaesthetic.
Rare or very rare complications
- Serious allergic reactions to drugs and death is very rare.
- If you have had a general anaesthetic, there is a very small risk of damage to eyes and vomit getting into your lungs.
- If you have had a spinal, epidural or nerve block, damage to nerves may occur, though it is uncommon. This can lead to an area of numbness, weakness, or pain in the legs. Usually this is temporary, although very rarely a serious, permanent injury can occur.
Coughs and colds
Although anaesthesia is very safe, it becomes significantly riskier if carried out when you are suffering from a cold or flu. If you develop a cold in the seven days before your admission, your surgery may be postponed but this will depend upon the nature of your surgery and the severity of your symptoms. Please contact the pre-admission nurse for advice.
What to bring to hospital
You will need your toiletries, nightclothes and some loose fitting, comfortable day clothes. You will be expected to dress in comfortable day clothes during the day while you are in hospital. T-shirts and shorts are practical when doing exercises. You must bring flat, comfortable, supported shoes – no backless shoes/slippers or flip flops. We do not have wardrobes in the ward therefore it is important to keep your personal belongings to a minimal.
Also, make sure you bring your usual medicines and a small amount of money, but leave valuables or jewellery at home. You may want to bring a few books or magazines. You may also want to bring packs of antiseptic hand wipes, which you can use every time you go to the toilet, and also before and after meals.
You can start a checklist before you come into hospital.
| Remember to | Completed |
| Pack all medication in original containers | |
| Pack suitable day wear and night clothing and toiletries | |
| Bring usual walking aid and any dressing aids | |
| Arrange care for pets and family | |
| Arrange discharge plans – for example lift home | |
| Ensure you have enough medication and will not run out | |
| Remove loose rugs | |
| Move furniture or other hazards | |
| Move items regularly used to be easily accessible | |
| Prepare food and meals for your convenience once home | |
| Freeze milk and bread for the first few days once home |
The day of surgery
The majority of patients are admitted to hospital the morning of surgery however some patients are admitted the day before. Your surgeon and your anesthetist will make this decision and discuss it with you.
Before arriving at hospital
Before a planned admission, you should have a long hot soapy bath or shower. But remember not to use talcum powder or heavily scented brands of soap. Have an all-over scrub with a soft gentle brush, exfoliator or loofah. Clip your toe and fingernails (removing all nail polish) and wash your hair.
Put on freshly laundered underwear. All this helps prevent unwanted bacteria coming into hospital with you and complicating your care.
Plants and flowers are not permitted in the ward due to infection control. Please remind your family and friends not to send flowers during your inpatient stay.
Have nothing to eat or drink (nil by mouth or fasting). You will receive clear instructions about fasting. It is important to follow these or your surgery may be cancelled. Food or liquid in your stomach during your anesthetic can come up into the back of your throat and damage your lungs. Even if you are not having a general anesthetic, you will still be asked to follow these instructions.
Take your normal medication. If you are taking medicines, you should continue to take them as usual, unless your anesthetist, surgeon or pre-operative assessment pharmacist has asked you not to.
Arriving in hospital
When you arrive, we will attach an identification bracelet to your wrist and a nurse will complete any final paperwork. A member of the orthopaedic and anaesthetic team will also see you and check your consent. They will mark your operation site with a marker pen.
Please note that once your admission is completed, you may have a long wait depending upon where you are on the theatre list, and you should bring something to read with you. Depending on where you are admitted to you will either be allocated a bed or you will be in a sitting area.
Wherever you are, you will be kept informed and comfortable.
Anaesthetic review
Your anaesthetist will visit you before your operation and will ask you again about your health and discuss the anaesthetic and pain relief techniques suitable for you, together with their advantages and risks. You will have the opportunity to ask final questions and tell the anaesthetist about any worries that you have.
Glasses, jewellery or dentures
You can wear your glasses, hearing aids and dentures until you are in the anaesthetic room. If you are having a local or regional anaesthetic, you may keep them on. You should remove jewellery and decorative piercing beforehand.
In the anaesthetic room
This is the room next to the operating theatre. Several people will be there, including your anaesthetist and an anaesthetic assistant.
There will be equipment to measure:
- Heart rate: You will have three sticky patches on your chest linked to the electrocardiogram (ECG).
- Blood pressure: You will have a cuff on your arm.
- Oxygen level in your blood: A clip will be placed on your finger or ear (pulse oximeter).
A needle is used to put a thin soft plastic tube (a cannula) into a vein in the back of your hand or arm. Drugs and fluids can be given through this cannula.
During the operation
You will then either walk or be wheeled into the operating room (theatre) and transferred onto the operating table and positioned. The dedicated orthopaedic team will be in theatre to ensure your operation runs smoothly. All anaesthetics may cause changes in your heart rate, blood pressure and breathing. Your anaesthetist may intentionally adjust these to control your response to surgery. Anaesthetic drugs are given continuously throughout surgery and are stopped when the operation ends.
An anaesthetist will stay with you for the whole operation and watch your condition very closely, adjusting the anaesthetic as required. If you have opted for a regional anaesthetic you may hear people talking, machines bleeping and surgical instruments making loud noises. These are all normal parts of your operation. Please discuss this with your anaesthetist if this concerns you.
Blood transfusion
You will lose blood during and briefly after your operation. Your body can normally cope with this and produces more blood over time to replace the lost amount.
Every effort will have been made to minimize blood loss during surgery but on occasions after your operation you may have a low blood count. This can make you feel lightheaded and dizzy. There are options for treatment including an iron infusion or blood transfusion if needed. This will be discussed with you.
After your surgery
Following your surgery you will be taken to the recovery room, near the operating theatre and a recovery nurse will look after you. You will not be left alone and there will be other patients in the same room.
You may need to breathe oxygen through a mask and you will have a drip – a bag of fluid attached to your cannula which drips slowly into a vein. Your blood pressure, heart rate and oxygen level will be measured. If you have pain or sickness, the nurse will treat it promptly. If you have any pain at this stage, you must let the recovery nurse know, as this is the best way your pain can be assessed and controlled.
Nursing staff will check the wound on your knee regularly. If you have had a spinal anaesthetic you may not be able to feel your legs or be aware when you are passing urine. This is normal, and the sensation will come back once the anaesthetic wears off. Some people have difficulty passing urine following a spinal anaesthetic. If this is the case the nurses may put a catheter in for a short period of time until your bladder control returns to normal.
Pain relief
Good pain relief is essential to help you recover quickly from your surgery. Some people need more pain relief medicines than others. The nurses will reassess the degree of pain you may have. Be honest with your answers. An assessment scale is used to measure your pain regularly. The nurses will ask you to rate your pain at rest and on movement. They may use a numeric scale of zero to ten – zero meaning no pain and ten being severe pain. You may also choose the word that best describes your pain:
For example, no pain, mild, moderate, severe or worst pain ever. Whichever tool you use, it is important that you are honest about your pain so that you can receive the appropriate treatment for you. It is vital to the success of your joint replacement that you are not inhibited from exercising because of your pain.
For pain relief, we may give you:
- Tablets or liquids to swallow: You will be given more that one type of painkiller in order to relieve your pain and can be increased in strength if required. They take at least half an hour to work and you need to be able to eat and drink and not feel sick for these drugs to work.
- Injections: These are given into a vein for immediate effect, just under the skin or into your thigh or buttock muscle. Strong pain relieving drugs, such as morphine, pethidine and tramadol may be given by injection.
Nausea
There is a risk that you may feel nauseous following your surgery. It is important that you mention this to the nursing staff as soon as possible so that they can give you something to help combat this. The nurses are there to reassure you. Do not be afraid to ask them things you are not sure of.
Nerve blocks and epidurals
These can give effective pain relief for hours or days after the operation. When the sensation begins to return and numbness wears off, you must inform the nurse who will give you suitable painkillers.
Occasionally, despite regular painkillers, you may experience stronger pain. This may occur during physiotherapy exercises or when walking. You will have additional painkillers prescribed to help relieve this pain but you will need to ask your nurse for these. It is important that you are comfortable enough to be able to comply with physiotherapy for your optimum recovery and to prevent any delay in discharge. Do not wait to be asked and do not feel afraid of being a nuisance. If your pain is effectively controlled, post-operative complications are reduced. Good pain control will allow you to sleep better, help your body heal more quickly and enable you leave hospital sooner.
You can get more information about pain relief from:
- the nurses on the ward
- your anaesthetist
- acute pain team – this is a team of nurses and doctors who specialise in the relief of pain after surgery
Back on the ward
Following your operation and recovery, you will be taken in your bed back to the orthopaedic ward. The nursing staff will look after you for the rest of your time in hospital.
You will be connected to various pieces of equipment. This is normal. These machines help the nurses monitor your blood pressure and pulse. You may have oxygen through a mask or small tubes into your nostrils.
Depending on the time of your operation the ward staff will encourage you to start gentle exercises and will help you to move from the bed to the armchair with a walking frame. Most patients will be able to walk on the same day as their surgery. This early movement promotes good circulation and movement of your knee. Being in a more upright position will also help reduce the risk of chest complications.
The day after your operation
- We will take a blood sample.
- You may still be connected to various pieces of equipment – this is normal.
- We will ask you to wash and dress in comfortable day clothes – loose fitting shorts/skirt.
- We will encourage you to sit out of bed for your meals.
- You may have an x-ray but you can still mobilise and do your exercises before this is done.
- You may not feel like eating much on this first day, but it is important that you drink little and often.
- You can sit in a chair and can walk to the toilet.
Cryocuff therapy
Cryocuff therapy is a cold compression system to minimise swelling, bruising and pain. This is very important for your rehabilitation. It is fitted by the physiotherapist. It should be used as often as you wish whilst resting and sleeping, and removed when you are exercising or walking.
The cryocuff consists of two parts: a blue cuff which fits around your knee, and a bucket filled with ice and cold water.
The cuff is filled with the cold water by attaching the bucket through a plastic tube, to the cuff. You should lift the bucket above the cuff to fill it, or place the bucket below the cuff to empty it. Your physiotherapist will teach you how to apply, fill and empty the cuff yourself.
At first, rechill the water in the cuff after 15 or 30 mins, then once an hour as needed. The ice in the bucket needs replenished every 6-7 hours to keep the water in the bucket cool.
Using your cryocuff, elevating your leg when sitting, and doing your exercises regularly will all help to speed up your recovery.
When you are discharged, you can take the water-filled cuff home, and use it like a cold pack.
Place the cuff in a bag and put it into the fridge to cool. Do not keep it in the freezer, as this cools the cuff too much.
Occupational therapy following your knee replacement
A member of the Occupational Therapy team will speak with you after surgery to promote independence with everyday activities and address any concerns that you may have.
Physiotherapy following your knee replacement
Physiotherapy is crucial to your rehabilitation following your operation. In order to get the best physical results from your joint replacement, it is extremely important that you follow the instructions and advice given by the physiotherapy staff.
Common terms used in physiotherapy:
- Extension: straightening action of the knee
- Flexion: bending action of the knee
- Quads: large muscles at front of thigh to straighten the knee
- Hamstrings: large muscles at back of thigh to bend the knee
Exercises after your surgery
We will teach you a series of exercises to increase the movement of your joint and to strengthen the muscles around the knee. This will also help reduce swelling and pain. We advise that you take enough pain relief to allow you to perform your exercises. The following exercises can be started at home, before you come in for your operation and also good to start a few hours after your operation. They should be practiced three to four times every day; increasing the number of repetitions as indicated by your physiotherapist. You must take responsibility for your own exercises outwith physiotherapy sessions.
When performing any exercise, maintain a comfortable upright posture and keep your breathing regular.
It is expected that you will need to carry out all the exercises described below. However, there may be an occasion when you might have to omit a particular exercise. Your physiotherapist will advise when and why this is appropriate.
Moving around
It is important to become mobile quickly following your operation. This will help prevent circulation complications, as well as being good for your whole body in general. You may be out of your bed a few hours post surgery. Initially you may need a walking frame to help you walk.
Standing up safely when using a walking frame
- Move to the edge of the bed or chair.
- Keeping feet hip width apart, bring them back as far as is comfortable. Your operated leg may not bend as far as your other leg.
- Place your hands on the bed beside your hips or on the arms of the chair.
- Lean forwards, push down on your hands and stand up.
- Now take hold of your walking frame and stand up straight.
Standing up safely when using walking sticks or elbow crutches
- Move to the edge of the bed or chair.
- Keeping feet hip width apart, bring them back as far as is comfortable. Your operated leg may not bend as far as your other leg.
- Place your sticks or crutches in the hand on the same side as your operated knee.
- Place your other hand beside your hip or on the arm of the chair.
- Lean forwards, push down on your hands and stand up.
- Take a crutch or stick into each hand: your physiotherapist will further explain how to do this.
Sitting down
- Before sitting, make sure you can feel the bed or chair behind your legs.
- If using a walking frame, reach down and back with your hands to feel for the bed or chair.
- If using crutches or sticks, take them across to the hand on your operated side and reach down and back with your other hand to feel for the bed or chair.
- Bend your knees, stick your bottom out and ease gently down to sit.
Walking
It is essential you achieve a normal walking pattern and your physiotherapist will work with you to achieve this.
The technique is to place your walking aid forward, step with your operated leg, control your knee by tightening your thigh muscles, lean through your hands onto your walking aid, then step through with your other leg. When walking with sticks, you should use them with the handle facing backwards. When you have progressed to one stick, hold it in the hand opposite the affected leg. Walk placing the stick on the ground at the same time as the affected leg.
Stairs
We will show you how to go up and down stairs safely and how to protect your knee when doing so. Stairs practice is necessary for everyone – even though you may not have stairs at home, you will have to negotiate kerbs or stairs outwith your own home.
Going up
- Use handrail if available
- Step up with unoperated leg (think “Good” Leg goes up to heaven)
- Follow with operated leg onto same step
- Bring up the crutch or stick onto same step
Going down
- Use handrail if available
- Place crutch or stick down onto step
- Step down with operated leg onto same step (think “bad” leg goes below)
- Follow with unoperated leg onto same step
Continuing physiotherapy at home
You must continue with your exercises at home every day, two to three times a day. You will also attend a weekly knee exercise class for up to six weeks – we will arrange an appointment for this before you go home. Gradually increase your walking distance with your sticks or crutches. The physiotherapist at your class will advise you when to start using only one stick or crutch and progress to walking with no aids.
Discharge
You will be able to go home from hospital two or three days after your operation, some people go home the day after their operation. This will only happen if you and the team looking after you think it is safe for you to do so.
Before you go home, we will give you advice on any new tablets, such as painkillers and when to start any tablets that were stopped.
Your medication will be returned to you. However, you may require to contact your family doctor (GP) for a ‘top-up’ of medication.
You will return to the clinic around six to eight weeks following surgery. You will be seen by the orthopaedic specialist nurse. No x-ray will be required. You will have an x-ray organised at your nearest x-ray department one year after surgery.
Activities to do after discharge
During the first six weeks you should concentrate on the exercises shown to you, and take regular short walks.
You can progress to using one stick when you can walk comfortably without a limp. Use one stick in the opposite hand to the side of surgery. You can progress to no sticks when you can do this without a limp. This will be at around four to six weeks but on some occasions can take longer.
Work
It is normal to take 3 months off from work, but you can return as soon as you are comfortable. Timing of returning to work depends on what activities are necessary for your work.
This is something to discuss with your consultant at your review which usually occurs at 6 weeks following your surgery.
Sport and leisure
Return to low impact sporting activity may take 3 months. Remember when you resume sport that you will not be able to perform as the same level initially.
The safest aerobic exercise is cycling (stationary or traditional) because it places very little stress on the knee joint. Consult your surgeon before beginning any new sport or activity.
Driving
Follow your surgeon’s advice about driving. You should not drive until you are confident that you could perform an emergency stop without discomfort. This will be after around 6-8 weeks.
Activities to avoid
Following a total knee replacement, high-demand or high-impact activities must be avoided.
It is not advisable to kneel after a total knee replacement, but this is acceptable following a half knee (partial) replacement.
It is also advisable to avoid repetitive heavy lifting. These activities put too great a strain on the artificial joint and could cause it to become loosened over time.
Maintaining appropriate weight will also help to reduce wear on your total knee replacement. Use the NHS body mass index (BMI) calculator to help you.
Outpatient physiotherapy
You will normally be offered an outpatient physiotherapy appointment after you have been discharged from the hospital, usually within 2 weeks after leaving hospital. There are different ways your appointment may take place:
- Telephone Appointment
- Virtual Consultation via Near Me (Attend Anywhere) – see our total knee replacement information leaflet for more details.
- Face-to-Face if having difficulty that has not been resolved from telephone or virtual
The physiotherapy will then modify your rehabilitation programme and exercises to help you regain range of motion in the knee and build strength in the muscles which support the knee.
Conclusion
After your knee replacement surgery and rehabilitation, your knee should have a range of motion of anywhere between 0-120 degrees, sufficient for all your daily tasks.
Thanks to your new knee, you will be able to do many of the activities you did before your knee surgery, but with little or no pain. Most people with total knee replacements can do recreational walking, swimming, golf, driving, light hiking, recreational biking, ballroom dancing and stair climbing without difficulty.
Read our printable information booklet regarding knee replacement surgery.
Knee: joint replacement exercises
The exercises in the videos below have been provided to help with your knee pain as you recover from your surgery. If there is any doubt about your fitness to do these exercises then please discuss this with your GP or consultant.
You may find that these exercises may slightly increase your symptoms initially. However you should find that the exercises themselves will become easier to do and that you begin to move your knee more easily. It can take around 12 weeks for you to notice a great improvement.
If the exercises do cause some discomfort, then taking prescribed medication from your GP or pharmacist may help you to continue to exercise.
If these exercises cause a large increase in your pain, or after 12 weeks there are no noticeable changes in your day to day symptoms, please contact your GP or NHS Inform for more advice.
The guide below will help ensure you are working at the right level.
Pain during exercise
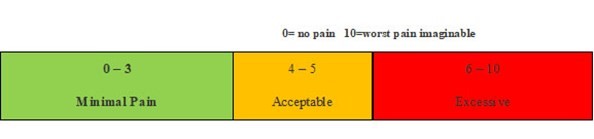
Within the scale, aim to stay in the green or amber boxes. If you are in the red area then you can modify the exercises by:
- reducing the amount of movement during an exercise
- reducing the number of repetitions
- reducing the weights
- reducing your speed
- increasing rest time between sets
Pain after exercise
Your pain or other symptoms should return to your pre-exercise baseline within 30 minutes of exercising. On the morning after your exercises, you should not feel an increase in pain or stiffness that lasts longer than 60 minutes.
Disclaimer
Please note: These exercises should not be used without prior consultation with a medical professional as the use of the wrong exercise may cause additional health related issues and discomfort. NHS Ayrshire & Arran and MSK NHS Ayrshire & Arran are not liable or responsible for any harm, losses or damages whatsoever resulting from the use or misuse of the information contained in or implied by the provided information in each video. These are provided for information only.
If you have any concerns about your ability to perform exercise then please discuss your concerns with your doctor or healthcare provider prior to participating in any advice that is on the MSK NHS Ayrshire & Arran website.
It is recommended to use your ice pack (cryocuff) or cool pack after your exercises to reduce the pain and discomfort this may cause.
Please choose the most relevant exercise section for you.
Section 1: Mobility Exercises
After a Total Knee Replacement it is important to improve range of movement at your knee once discharged home.
To be able to achieve full straightening of your knee and to encourage the bend at your knee it is important to regularly do mobility exercises during your recovery.
Exercise 1: Knee Flexion
To do this exercise – Sit in bed with your operated leg out straight in front of you. Use your heel on the bed to gently bend your knee up as far as you are able. Then straighten knee back to starting position. Repeat for 30-60 seconds. Aim for 3 sets daily.
To help increase your movement further when bending knee upwards, use your hands to gently to pull your knee towards you to get a larger bend. Hold the knee bent for 5 seconds. Then slide heel back down bed to starting position.
This exercise can feel uncomfortable initially. Overtime it will feel more comfortable to bend your knee and you will notice an improvement in the movement.
Exercise 2: Ankle Dorsiflexion and Plantarflexion
It is also important for regularly mobilising your ankles when recovering from your operation. This will also promote good circulation.
To do this exercise lie or sit in bed with legs straight. Move your ankles forward and backwards together, or alternate legs.
Repeat for 20 repetitions, 3 times per day.
Exercise 3: Heel and Toe Raises (Seated)
To do this exercise, sit comfortably in a chair with feet flat on the floor. Lift both heels up from the floor then lower down to the starting position. Then pull your feet upwards to the ceiling and then back flat.
Repeat for 20-30 repetitions, 3 times per day.
Exercise 4: Active Assisted Knee Flexion and Extension
To do this exercise sit on a chair with a plastic bag under the foot of your operated leg. Slide your heel back to bend your knee as much as you can then slide your foot forwards to fully straighten the leg.
Repeat for 30-60 seconds.
This exercise is beneficial to do every 1 to 2 hours to help decrease stiffness in the knee particularly when you are spending long periods sitting.
Section 2: Strengthening
An important component of your recovery after a Total Knee Replacement is to strengthen your thigh muscles. This will help regain your function and help improve your mobility.
At first you may find some of the exercises uncomfortable however as you become stronger and fitter, they will feel easier to do.
It is important to aim for 3 sets of each exercise daily.
Exercise 1: Static Quadriceps Contraction
To do this exercise – Start by either sitting or lying with your operated leg out straight in front of you. Tense your thigh muscle by pushing the back of your knee down into the bed. Hold for 5 seconds. Then relax.
Repeat for 10 repetitions. Aim to do at least 3 sets per day.
Exercise 2: Static Quadricep Contraction with Towel Support
To do this exercise - sit or lie in bed with your operated leg straight out in front of you. Have a rolled-up towel under your ankle. Push the back of your knee down to the bed and pull your ankle up towards your head. Hold for 5 seconds then relax.
Repeat for 10 repetitions. Aim to do at least 3 sets per day.
Exercise 3: Static Quad Contraction with Stool Support
To do this exercise – sit on a chair with your operated lower leg resting on a stool. Try and then straighten your leg as much as possible as if pushing the back of your knee down towards the floor. Pull your foot up to your head. Hold for 5 seconds then relax.
Repeat for 10 repetitions. Aim to do at least 3 sets per day
Exercise 4: Perched Sitting Quadriceps Contraction (Static)
To do this exercise sit on a chair. Slide forward so that you are slightly perched off the chair. Have your operated leg stretched out straight in front of you and have your heel resting on the floor. Tense up the thigh muscle (quadriceps) as if pushing the back of your knee towards the floor. Hold for 5 seconds then relax.
Repeat for 10 repetitions. Aim to do at least 3 sets per day.
Exercise 5: Inner Range Quadricep Contraction
To do this exercise – Sit up in bed with a rolled-up towel under your knee. Straighten your knee keeping the back of your knee on the towel. You should feel the front of your thigh muscles working as you hold your knee straight for 5 seconds. Then return to starting position.
Repeat 10 repetitions. Aim to do at least 3 sets per day.
Exercise 6: Straight Leg Raise
To do this exercise - Sit or lie in bed with your operated leg straight out in front of you. Pull your foot upwards to point towards your head. Keep your leg straight and slowly raise your leg up off the bed by about 20cm. Hold this position for 10 seconds before lowering to the starting position.
Repeat for 10 repetitions. Aim to do at least 3 sets per day.
Exercise 7: Seated Knee Extension
To do this exercise – Sit on a chair with your feet on the floor. Slowly straighten your operated leg, once it is fully straight, pull your foot towards your head and hold for 5 seconds. Then bend knee and return to the starting position.
Repeat for 10 repetitions. Aim to do at least 3 sets per day.
Section 3: Functional Exercises
An important part of your rehabilitation is including exercises that will help tasks of your daily living after your Total Knee Replacement.
Exercise 1: Mini Squats
To do this exercise – Stand holding the back of the chair for support. Slowly bend both knees and bring your bottom back as if doing a half sit down. Then return to standing position.
Aim initially for 10 repetitions as comfort allows. Aim to do 3 sets per day.
Exercise 2: Sit to Stand
To do this exercise – Start by sitting on a chair with arm support. Initially use your arms to help you stand up. On going to sit down step backwards so the back of your legs feel the chair behind them. Then slowly bend your knees and sit down. Aim for 10 repetitions.
Once you find this easier try this exercise without your hands. As time progresses try have equal weight through both legs during this exercise.
Once fitter and stronger try and aim for 3 sets of 10 repetitions daily.
Further support
Read our printable information booklet regarding knee replacement surgery.