

Trigger finger is a painful condition in which a finger or thumb clicks or locks as it is bent towards the palm.
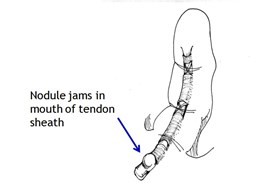
Diagram 1: Picture showing why Triggering can Happen
What is the cause?
Thickening of the mouth of a tendon tunnel leads to roughness of the tendon surface, and the tendon then catches in the tunnel mouth. People with insulin-dependent diabetes are especially prone to triggering, but most trigger digits occur in people without diabetes. Triggering occasionally appears to start after an injury such as a knock on the hand. There is little evidence that it is caused by work activities, but the pain can certainly be aggravated by hand use at work, at home, in the garden or when participating in sport. Triggering is sometimes due to tendon nodules in people known to have rheumatoid arthritis. It is not caused by osteoarthritis.
What are the Symptoms?
- Pain at the site of triggering in the palm (fingers) or on the palm surface of the thumb at the middle joint, usually in a person over the age of 40.
- Tenderness if you press on the site of pain.
- Clicking of the digit during movement, or locking in a bent position, often worse on waking in the morning. The digit may need to be straightened with pressure from the opposite hand.
- Stiffness, especially in trigger thumb where movement at the end joint is reduced.
Trigger finger/thumb – myths versus facts
Myth Everyone with Trigger finger needs an operation.
Fact The majority of Trigger finger/ thumb respond well to a steroid injection and most do not require surgery.
Click HERE for a printable version of this section
What is the treatment for a Trigger Finger or Thumb?
Trigger finger and trigger thumb are not harmful, but can be a really painful nuisance. Some mild cases recover over a few weeks without treatment.
The options for treatment are:
- Avoiding activities that cause pain, if possible.
- Using a small splint to hold the finger or thumb straight at night. A splint can be fitted by a hand therapist, but even a lollipop stick held on with tape can be used as a temporary splint. Holding the finger straight at night keeps the roughened segment of tendon in the tunnel and makes it smoother. See the diagram below in the splint section.
- Steroid injection relieves the pain and triggering in about 70% of cases, but the success rate is lower in people with diabetes. The risks of injection are small, but it very occasionally causes some thinning or colour change in the skin at the site of injection. There is also a small risk of infection causing swelling, redness and pain. Improvement may occur within a few days of injection, but may take several weeks. A second injection is sometimes helpful, but surgery may be needed if triggering persists. Click HERE for more information on corticosteroid injections.
- Surgery is considered when triggering does not resolve with steroid injections. The operation is usually done under local anaesthetic as a day case. The operation involves releasing of the tendon tunnel.
Splints for Trigger finger or thumb
As described in the previous section sometimes keeping the finger in a straight position during the night can allow any irritation or thickening which sits in and around the covering of the tendon to settle. You may have worked out yourself that keeping your hand flat under the pillow is helpful.
A home-made splint using a lollipop stick held on with tape can be effective.
There are also some simple splints available online like the one below.

Diagram 1: Example of Trigger Finger Splint
Unfortunately these are not something that are routinely issued by your family doctor (GP). We are not saying that you should rush out and buy this, we are simply giving you options of things which can be very helpful.
Click HERE for a printable version of this section