

Cubital Tunnel Syndrome
What is Cubital Tunnel Syndrome?
Cubital Tunnel Syndrome is compression or irritation of the ulnar nerve within a tunnel on the inside of the elbow behind a bone called the medial epicondyle (where your ‘funny bone’ is).
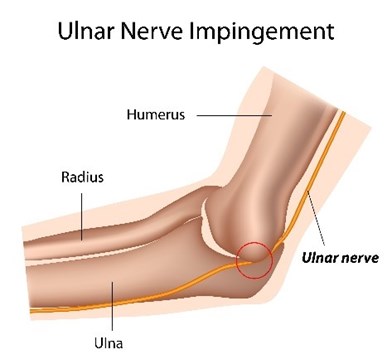
Diagram 1: Picture of Where the Ulnar Nerve Can be Compressed
The ulnar nerve is one of three important nerves for hand function. It enables feeling/sensation to the skin of the little finger and half of the adjacent ring finger, power to some of the muscles that bend the little and ring fingers and to some of the small muscles in the hand and thumb.
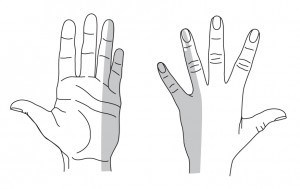
Diagram 2: Area of Where Altered Sensation Can Occur in Cubital Tunnel Syndrome
What are the symptoms of Cubital Tunnel Syndrome?
Pain, numbness and/or tingling of the little and ring fingers are usually the earliest symptom. It is frequently intermittent, but may later become constant in nature. Often the symptoms can be provoked by repetitive elbow bending and straightening, by leaning on the elbow or holding the elbow in a bent position (for example, on the telephone). Sleeping with the elbow habitually bent can also aggravate the symptoms. Some patients may also notice some weakness of pinch grip with their thumb.
In the later stages, the numbness is constant and the hand becomes weak. There may be visible loss of muscle bulk in severe cases, particularly noticeable on the back of the hand between the thumb and first finger, with loss of strength and dexterity.
What causes it?
Cubital Tunnel Syndrome is the second most common entrapment neuropathy in the human body. Most cases arise without an obvious cause, but the tunnel can be narrowed by arthritis of the elbow joint or by an old elbow injury. Many patients develop symptoms as a result of overuse of the elbow, leaning on the elbow or from direct pressure over the ulnar nerve when using a computer at a desk.
As with all nerve disorders, patients with diabetes are at increased risk of ulnar nerve symptoms. Other factors associated with an increased risk of Cubital Tunnel Syndrome include wear and tear/inflammation of your tendons, hypothyroidism and obesity.
What is the natural history?
The symptoms of Cubital Tunnel Syndrome generally come and go and rarely affects the ability to carry out activities involved with daily living. The condition will often settle completely with simple measures such as avoiding direct pressure on the nerve and avoiding prolonged full flexion of the elbow.
Diagnosis of Cubital Tunnel Syndrome
Diagnosis can often be made from the clinical history (the account of events and symptoms from the patient) and a clinical examination of the elbow and hand. The examination will assess for muscle weakness, irritability of the nerve to tapping and/or bending of the elbow, and changes in sensation. Other medical conditions may need to be evaluated such as thyroid disease or diabetes. A test called electromyography (EMG) and/or nerve conduction study (NCS) may be done to confirm the diagnosis of Cubital Tunnel Syndrome and determine its severity.
Myths versus facts
Myth If I have Cubital Tunnel Syndrome I will need an operation
Fact The symptoms usually settle on their own or with simple advice and exercise. It is relatively rare that surgery is required.
What is the treatment?
Avoiding or modifying any activity which aggravates your symptoms is the main treatment in the early stages and may significantly reduce the pressure on the nerve. This should include a workstation assessment. For example, wear a headset for using the telephone, place computer keyboards at the edge of the desk and use a chair that does not have an arm rest.
Prolonged flexion (bending) of the elbow should be avoided and any activity that puts direct pressure on the nerve should be modified. Avoid leaning on the inside of the elbows and wearing an elbow pad over the ulnar nerve and “funny bone” may help.
Splint
Excessive bending of the elbow at night can be minimised by wrapping a folded towel around the elbow or by wearing a splint.

Diagram 3: Towel Splint for Cubital Tunnel
Try using the splint during periods of rest and also at night whilst in your bed. This needs to be attempted for at least 3 months before an understanding if this is helping your symptoms.
Click HERE for a printable version of this section.
Exercises for Cubital Tunnel Syndrome
‘Tendon Glides’
The following exercises have been suggested as being helpful in improving the movement of the tissues in and around your elbow. Learn the sequence of moving through positions one to four. Once you have learned the sequence, this should be repeated 10 times. Aim to do these exercises little and often throughout the day, for example, three or four times a day.

Diagram: Tendon Glide 1

Diagram: Tendon Glide 2
Neurodynamic
Exercise 1 – Ulnar Nerve Gliding
To do this exercise – stand with your affected arm at 90 degree shoulder flexion. Wrist in extended position with palm facing up towards the roof. Side flex your head away from arm as you extend elbow so that your palm faces towards the roof then return to the starting position.
Do for 30 seconds, repeat several times per day.
Click HERE for a printable version of this section.
Other treatments – general advice
Surgery for Cubital Tunnel Syndrome
As we have mentioned previously, surgery to decompress the nerve (relieve pressure) may be required in severe cases, or in those that do not respond to the non-surgical treatments above. Surgery frequently improves the numbness, but its main objective is to prevent the progressive muscle weakness and wasting that tends to occur in severe untreated cases. Surgery is rarely required and usually you would have to go for special tests on your nerves, called nerve conduction studies, before this is considered.
What is the outcome?
The outcome of surgery depends upon the severity of the compression being treated. Numbness frequently improves, though the improvement may be slow. Surgery generally prevents worsening of the muscle weakness, but improvements in muscle strength are often slow and incomplete.
Surgery does not help if the cause of your symptoms are related to posture and positioning. Therefore, if you have been given this advice it very important that you work on improving this to the best of your ability.
Click HERE for a printable version of this section