
The anatomy of the knee
The knee is a hinge joint formed by the:
- tibia (shinbone)
- femur (thighbone)
- patella (kneecap)
The ends of the bones in the joint are covered with cartilage. Cartilage is a tough lubricating tissue that helps cushion the bones during movement.
The joints
The joint mainly allows for bending (flexion) and straightening (extension) of your knee. The knee joint consists of two articulations-tibiofemoral and patellofemoral. The joint surfaces are lined with cartilage, and are enclosed within a single joint cavity.
Tibiofemoral (knee joint) – medial and lateral condyles of the femur articulate with the tibial condyles. It is the weight-bearing component of the knee joint.
Patellofemoral (kneecap) – (anterior) aspect of the femur at the knee joint articulates with the patella. It allows the tendon of the quadriceps femoris (muscle that extends knee) to be inserted directly over the knee, increasing its efficiency.
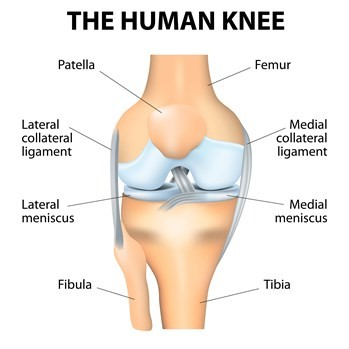
The ligaments
There are a number of ligaments related to the knee. However the main ones are the collateral and the cruciate ligaments. These ligaments work to stabilise the knee and give the knee its awareness of its position in space.
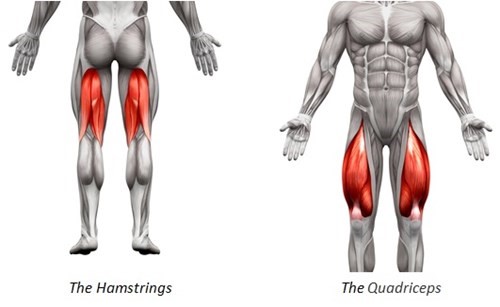
The muscles
The main muscles of the knee joint consist of two groups that work together to extend and flex the knee joint during activities such as walking and running.
The muscles at the front of the thighs are called the quadriceps. They are a group of four muscles which work to extend or straighten the knee. They attach to the shin bone by a thick tendon called the patellar tendon.
At the posterior aspect of the thigh are a group of three muscles called the hamstrings. They work together to flex the knee during activities.
These are the main muscles which directly control the knee. However other muscles such as the gluteal muscles are important to help control the position and alignment of the knee. Remember: general muscle conditioning is also important!
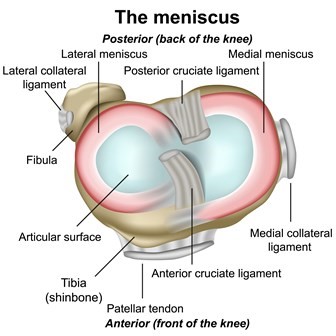
Menisci
The menisci are C-shaped tissues inside the knee joint, located between the thigh (femoral) and shin (tibia) cartilage surfaces. Both are found in the joint. There is one on the inside of the knee (medial) and one on the outside (lateral).
The outer parts have adequate blood supply, but the middle and inner parts have poor blood supply. Because blood supply can affect healing, the location of a tear will affect treatment options.
What does the meniscus do in your knee?
The menisci are tissues that respond to the forces and loads that you put into the knee. They have several important functions:
- shock absorption
- load transmission (spreading weight more evenly into the knee joint)
- increasing knee joint stability
- joint lubrication
Common myths about knee pain
Myth 1: “A scan will explain my level of pain and disability”
Fact: It is common for patients to believe that the amount of damage seen on a scan such as an X-ray is directly related to the amount of pain and disability a person has. Research suggests this isn’t the case.
Structural changes play a role but the amount of degeneration does not correlate with pain or disability and there are other factors which also contribute to each person’s experience of pain
Myth 2: “Exercise is bad for my knee”
Fact: Exercise is in fact very good for your knee and is recommended as a safe and effective treatment for all persons with knee pain and osteoarthritis. There will be differences regarding the amount and intensity of exercise that an individual can tolerate. It is important that you get into a regular routine.
Myth 3: “Rest will help with my pain”
Fact: Rest used to be prescribed for knee pain. In most instances, rest and avoidance of exercise makes pain worse – especially in the long term.
Myth 4: “Surgery is the answer to my knee pain”
Fact: Guidelines suggest that surgery should be a last resort treatment for those who have not responded to prolonged conservative management. For example, we know 10% of those undergoing knee replacement continue to have pain.
Myth 5: “Pain means I am damaging my knee”
Fact: The most important thing you should know is that pain does not always mean harm. We can experience pain as a result of tissue damage, however it’s also possible to feel no pain with damage to our body. It’s also possible to experience significant amounts of pain even when no damage to our bodies has been shown.
What influences pain?
We know now that pain is far more complex than solely what is going on in our bodies and can be influenced by other areas of your life. These include:
- mood and emotions
- beliefs about pain
- avoidance of meaningful activities/social contact.
- lifestyle choices
This often referred to as the ‘biopsychosocial model of pain’ – meaning all areas of your life can influence pain. It is important therefore to look at your life as a whole when dealing with knee pain, to see if there are any other contributing factors.
See our Pain Management Service section for further information on understanding pain.
What can I do to help myself if I have knee pain?
There are lots of things you can do to help manage your symptoms. The best person to help is you. Changes in lifestyle and modifying your activities can reduce your symptoms and stop things getting worse.
Try not to worry – it is only natural to feel worried. Feelings such as worry, anxiety and fear, or negative expectations about treatment, can be barriers to recovery.
Weight management
Weight management is seen as the main long term management approach for knee pain. The only person that can maintain a healthy weight is you.
You can use the NHS Body Mass Index (BMI) calculator to work out whether your weight is healthy.
Researchers say that being overweight or obese can not only increase your risk of developing osteoarthritis, but will also make it more likely that your knee pain will get worse over time.
Losing even a small amount of weight can make a big difference to the strain on your joints, muscles, ligaments and tendons when walking, running, or going up and downstairs. There is no special diet shown to help knee pain but you should follow a balanced, low calorie-diet combined with exercise (such as walking, swimming or cycling).
You can access classes to help you with weight management:
Exercise
It is very important that you keep moving. You will need to find the right balance between rest and exercise. It is common that being over active can increase your pain but too little can stiffen up the joint. Two types of exercise can help your symptoms: strengthening and aerobic.
Strengthening exercises will improve the strength and tone of the muscles that control the affected knee. Pain and swelling from the injury process can weaken your thigh muscle (known as your quadriceps) resulting in your knee joint and structures taking more force. By regularly doing strengthening exercises this will help protect the joint and can be shown to reduce your pain.
Aerobic is any low to high impact physical exercise that makes you short of breath. This can help reduce pain by stimulating your pain relieving hormones called endorphins. There are a variety of different types of exercise that you can do, such as swimming, cycling or walking.
If you are not used to being physically active, it is best to speak with your GP to make sure your health allows you to undertake this type of self-management. If you are okay to participate in aerobic exercise, you may need to take a painkiller beforehand to avoid increased pain.
Condition-specific exercises
Local NHS Ayrshire & Arran physiotherapists have devised exercise programmes from the recent available evidence to help you improve your symptoms. Each knee condition will have its own suggested exercises. If you are unsure, please ask your GP or physiotherapist for advice for what exercises to attempt:
See our exercises for each condition:
- Knee Osteoarthritis
- Patellofemoral Pain Syndrome
- Knee Joint Replacement
- Degenerative Meniscal Tear Exercises
Painkillers
A range of different medications may be available to help reduce your pain to allow you to move more comfortably.
Do not exceed the daily allowance of these medicines, even if your pain is high.
Always consult a health professional prior to taking any new medication. If you are unsure of what medication you can take, speak with your local pharmacist, practice nurse or GP for guidance.
It is important that if you are prescribed medication that you take them regularly and at the recommended dose. See your medication packet for details.
All medicines can cause side effects, particularly if they are not used as prescribed. Side effects range from common to uncommon and vary from person to person. Information on possible side effects are available on the leaflet inside the packaging of your medication. If you experience side effects, it is important to speak to your local pharmacist, practice nurse or GP. They may be able to change the dose or the medication itself to something that is more suitable.
You should try and use the prescribed medication regularly at the recommend dose as prescribed. Some medicines can take a number of weeks to have significant effect, however this is dependent on the person. It is best to speak again with your GP or pharmacist about what other options are available if you don’t feel your medicines are helping.
Heat or ice
A hot water bottle or ice pack (such as a bag of ice cubes) can also be used regularly to help control pain after you have been overactive.
If using ice, wrap the ice pack in a towel and apply to the painful area for 10 minutes every two hours.
If you are using heat, wrap the warm compress in a towel and place it on the painful area for 20 minutes every two hours. If you have any concerns about the sensation or feeling on the skin where you are placing any of the mentioned compresses, ask your family doctor (GP) to assess this before following this advice. If you have any concerns that an infection may be present in the area then speak with a local pharmacist or GP prior to carrying out this advice.
Pace yourself
If you are in pain don’t tackle all your activities of daily living, such as housework, at once. Break the harder jobs down into smaller time frames and do something gentler in between.
Sometimes a short rest when your knee starts to feel painful can be helpful over the course of a day. It is recommended to pace rather than to fully stop all forms of movement or exercise.
You may find that taking simple painkillers as previously mentioned may help you to keep active.
Appropriate footwear
Avoid high heels. These:
- will alter the position of your leg
- can increase the strain into your knee and big toe
Daily aids
When climbing stairs you may need to consider using handrails and go up one leg at time until your muscles become stronger. It is better to go upstairs leading with the non-painful leg one step at a time. If coming down the stairs then lead with the sore leg one step at a time and use the handrail.
Using a walking aid such as a stick may be of benefit. This can be used to take the amount of weight going through the knee joint especially during a painful episode. If you are using a walking stick then ensure you are holding this on the opposite side from the painful knee. For example, if you have a painful right knee then hold the walking stick in the left hand.