

What is osteoarthritis?
Osteoarthritis (OA) is a condition that affects the joints causing pain and stiffness. The hip is one of the most commonly affected joints. Osteoarthritis is sometimes called ‘degenerative joint disease’ or ‘wear and tear’.
What happens in osteoarthritis?
Normal joints are constantly undergoing repair because of changes brought on by age. However, in some people, it seems that this repair process becomes faulty and osteoarthritis can develop. It is normal to expect some degree of osteoarthritis as we get older.
What causes osteoarthritis?
There are different factors that may cause OA.
Age
Osteoarthritis becomes more common with increasing age. By the age of 65 at least half of the people will have osteoarthritis in some of their joint(s).
Overweight
Hip osteoarthritis is more likely if you are overweight as increased load on the joints increases wear.
Gender
Women are more likely to develop osteoarthritis than men.
Genetics
Osteoarthritis is more likely if there is a history of joint problems in your family.
Previous joint damage or deformity
This may be from injury around the hip joint that has caused damage to the joint surfaces. There are some childhood hip conditions that can lead to OA in the future.
In many cases however, we do not know the exact cause of why osteoarthritis has developed and can be from a range of the factors discussed above.
What are the symptoms of hip osteoarthritis?
- Pain, stiffness and difficulty with movements of the joint is typical. The stiffness tends to be worse first thing in the morning but tends to loosen up after an hour or so.
- Pain, stiffness and weakness around the hips can lead to problems walking, putting on shoes and socks and activities such as getting in or out of the car. Eventually, pain can disturb your sleep.
- A locking or cracking sensation around your hip is fairly common.
You may experience all or some of these symptoms. Your symptoms may vary for no apparent reason with bad spells lasting a few weeks or months broken up by better periods with minimal pain or loss of function.
Is my pain coming from my hip joint?
Usually you feel osteoarthritis of the hip in the groin but it can also affect the front of your thigh and travel towards your knee.
Any pain in your buttock, side of your thigh or below the knee is unlikely to be coming from the hip joint itself.
Osteoarthritis of the hip does not cause altered sensation, pins and needles or cramping. If you have these symptoms then discuss with your GP/Practice Nurse or physiotherapist.
How do you diagnose osteoarthritis of the hip?
We usually diagnose osteoarthritis based on your symptoms and the physical signs we find when your Hip is examined.
X-rays can be used to confirm the diagnosis. However, in some cases this is not required.
What can I do to help myself?
There is no cure for arthritis , however there are many things you can do to manage your symptoms allowing you to maintain an active lifestyle. This will then help to reduce your pain and improve your function.
Reduce stress on the joint
- Keep to your ideal weight. Extra weight on your joint can make symptoms worse. You can use the Body Mass Index (BMI) Calculator to assess this.
- Wear footwear with cushioned soles or insoles.
- Try not to overstress your joint by doing too much all in the one day e.g. spread household chores throughout the week.
- Avoid being in one position for too long when possible to help prevent stiffness.
- Use a walking stick or walking poles if you find this useful.
Exercise
It is important to find the right balance between rest and exercise. Exercise in moderation can help to reduce pain, maintain function and possibly delay the need for a hip replacement. See our information on hip replacement surgery.
The goal is to find the correct balance between not doing enough exercise (which can lead to hip stiffness) and doing too much exercise (which might aggravate the symptoms). It is safe to continue high impact exercises if you are already able to do so. If you are struggling with weight bearing exercises you might try low impact exercise such as swimming, cycling, walking and aqua-aerobics.
Local physiotherapists have created exercises that can be used to help your symptoms, which can be found further down this page.
Medication
A range of different medications may be available to help reduce your pain to allow you to move more comfortably. Do not exceed the daily allowance of these medicines even if your pain is high and always consult a health professional prior to taking any new medication. If you are unsure of what medication you can take, speak with your local pharmacist, practice nurse or GP for guidance.
It is important that if you are prescribed medication that you take them regularly and at the recommended dose (see medication packet for details). All medicines can cause side-effects, particularly if they are not used as prescribed. Side-effects range from common to uncommon and vary from person to person. Information on possible side-effects are available on the leaflet inside the packaging of your medication. It is important to speak to your local pharmacist, practice nurse or GP who may be able to change the dose or the medication itself to something that is more suitable.
You should try and use the prescribed medication regularly at the recommend dose as prescribed. Some medicines can take a number of weeks to have significant effect, however this is dependent on the person. It is best to speak again with your GP or pharmacist about what other options are available if you don’t feel your medicines are helping.
Pace yourself
If you are in pain, don’t tackle all your activities of daily living (such as housework) at once. Break the harder jobs down into smaller time frames and do something gentler in between. Sometimes a short rest when your hip starts to feel painful can be helpful over the course of a day. It is recommended to pace rather than to fully stop all forms of movement or exercise. You may find that taking simple painkillers as previously mentioned may help you to keep active.
Daily aids
Use handrails
When climbing stairs you may need to consider using handrails. It is better to go upstairs leading with the non-painful leg one step at a time.
If coming down the stairs then lead with the sore leg one step at a time and use the handrail.
Walking aid
Using a walking aid such as a stick may be of benefit. This can be used to take the weight going through the hip joint especially during a painful episode.
If you are using a walking stick then ensure you are holding this on the opposite side from the painful hip. For example, if you have a painful right hip, then hold the walking stick in the left hand.
Heat and ice
A hot water bottle or ice pack (such as a bag of ice cubes) can also be used regularly to help control pain after you have been overactive.
If using ice, wrap the ice pack in a towel and apply to the painful area for 10 minutes every two hours.
If you are using heat, wrap the warm compress in a towel and place it on the painful area for 20 minutes every two hours.
If you have any concerns about the sensation or feeling on the skin where you are placing any of the mentioned compresses, ask a GP to assess this before following this advice. If you have any concerns that an infection may be present in the area then speak with a local pharmacist of GP prior to carrying out this advice.
Will I need surgery for my hip?
Surgery for hip osteoarthritis is usually with a total hip replacement.
Your healthcare team should always try other non-operative measures before suggesting a hip replacement. These may include weight loss, painkillers, use of a walking stick and activity modification.
Surgery is usually only performed in patients with moderately severe or severe arthritis on their x-rays.
Not everyone with osteoarthritis of the hip will feel their symptoms are severe enough to consider a hip replacement. If your symptoms are still manageable and your medication is effective then you may prefer to wait.
If you don’t want surgery for your hip osteoarthritis at this time then you don’t need a referral to hospital to see an orthopaedic surgeon.
If your hip has significant osteoarthritis and your day to day quality of life is significantly affected by pain, stiffness and disability, and despite trying all the advice in this leaflet we may consider you for a hip replacement.
Please note that 5-10% of patients who have hip replacement surgery are not satisfied with their hip replacement and a small number can develop serious complications as a result of the surgery.
See our information on hip replacement surgery.
Are there any reasons why I can’t have a hip replacement?
Unfortunately, some people may not be able to have a hip replacement even though their osteoarthritis is very bad.
This may be because:
- You have a serious medical condition
- You are at risk of falling
- You have deep or long-lasting open sores (ulcers) in the skin of your leg, increasing your risk of infection.
- You have other medical conditions that put you at higher risk from an anaesthetic.
It is important you are the best shape you can be prior to undergoing what is major surgery. As such if your weight is too high (BMI > 40) or too low (BMI < 20) this may need to be addressed prior to surgery. You can use the Body Mass Index (BMI) Calculator to assess this.
You can find help with weight loss here:
- East Ayrshire: Weigh to Go – East Ayrshire
- North Ayrshire: Weigh to Go – North Ayrshire
- South Ayrshire: Weigh to Go – South Ayrshire
If you are anaemic (too little iron in the blood) again this may need to be corrected prior to surgery.
If you are diabetic and your diabetic control is poor this again may need to be corrected.
What is a hip replacement and what risks are associated with it?
If your hip is damaged by arthritis and the pain, stiffness and disability are having a serious impact on your everyday activities and you have tried all the self help advice then the orthopaedic surgeons may offer you a hip replacement.
Hip replacement surgery is performed in ultra-clean theatres by a highly trained team of surgeons-anaesthetists-nurses and it is generally a very successful operation resulting in good pain relief and improved mobility.
During the surgery the hip is replaced with an artificial joint.
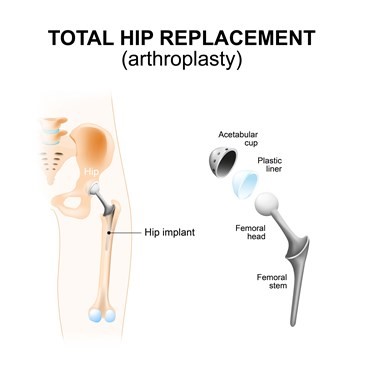
Procedure
The hip is the largest ball and socket joint in the human body and as such it can be prone to ‘wearing out’. Arthritis is painful and disabling and you and your surgeon may have decided that a hip replacement may be your best option if all measures have failed.
A hip replacement is a surgical procedure, in which the injured or damaged weight-bearing surfaces of the hip are replaced with artificial parts which are secured to the bone.
You will see the surgeon before your operation. You will also meet your anaesthetist who will discuss the type of anaesthetic with you. If you have any further questions that have arisen since your initial consultation this might be a good time to ask them. You will receive an anaesthetic in the theatre prior to your surgery commencing.
Your new hip will be checked with an x-ray after your operation (sometimes on the same day) and the inpatient physiotherapists will encourage you to stand and walk either on the day of surgery or at the latest by midday the day after the operation.
You will be in hospital for as long as it takes for you to be safe walking with sticks or crutches. It is important to note there will be discomfort after surgery of this nature and this is quite normal. Some patients will go home the same day as their surgery, some the following day and others slightly longer.
The physiotherapy team will visit you and demonstrate exercises. It is important to do these exercises (as pain allows). You can find exercises given to patients after undergoing hip replacement surgery further down this page.
What are the limitations after hip replacement surgery?
Generally you will be advised not to drive for at least 6 weeks. You would be best advised not to plan travel abroad for 3 months after the operation. A return to normal basic activities is likely between 6 and 12 weeks.
Risks
As with all surgical procedures, hip replacement carries some risks and complications.
- Pain: Your hip will usually be sore for a few days/weeks after the operation. If you are in pain, it’s important to tell ward staff so they can give you medicines. Pain will improve with time. Rarely, pain will be a chronic or long-term problem and may be due to some of the other complications listed below or for no obvious reason.
- Dissatisfaction: Although the majority of patients are happy following hip replacement surgery up to 10% of patients may experience some discomfort in their hip and may not be entirely satisfied with their hip replacement and up to 5% may feel that they are worse off.
Other common risks (occurs in 2-5% of those operated)
- Deep Vein Thrombosis (DVT): DVT is a blood clot in a vein. The risks of developing a DVT are greater after any operation (and especially a bone operation) DVT can pass in the blood stream and be deposited in the lungs (a pulmonary embolism – PE). This is a very serious condition which affects your breathing. Your surgeon may give you medication to try and limit the risk of DVTs from forming. And you may be provided with inflatable foot pumps to keep blood circulating around the leg. Starting to walk and moving about as soon as possible after your operation is one of the best ways to prevent blood clots from forming. The risk of DVT is increased in certain types of patient such as those with a family history of clots, those with other serious diseases such a kidney or liver disease and obesity. The biggest risk factors that you can do something about are obesity and smoking. You should try to address these risk factors before you even consider a hip joint replacement.
- Bleeding: Some patients may occasionally need a blood transfusion or iron tablets. Rarely, the bleeding may form a blood clot or large bruise within the hip which may become painful and may require an operation to remove it.
- Altered leg length: the leg which has been operated upon may appear shorter or longer than the other. This can affect up to 20% of patients and is occasionally managed with a heel raise on/in a shoe if it causes problems.
- Implant wear: With modern operating techniques and new implants, hip replacements last many years. However, in some cases, they may fail earlier. The reason is often unknown. The plastic bearing is the most commonly worn out part. If the replacement wears out or loosens it will become painful again and more surgery may be required. With newer designs of replacements however, wear is becoming less of a problem than it was in the past. Overall around 90-95% of hip replacement will last 10 years.
Less common risks (occurs in 1-2% of those operated)
- Infection: We will give you antibiotics at the time of the operation and the procedure will also be performed in sterile theatre conditions with sterile equipment. Despite this infections still occur (approximately 1 to 2% of cases). The wound site may become red, hot and painful. There may also be a discharge of fluid or pus. We usually treat this with antibiotics and an operation to wash out the joint may be necessary. In rare cases, the prosthesis may be removed and replaced at a later date. An infection can sometimes lead to sepsis (blood infection) and strong antibiotics are required in addition to further surgery. Weight loss and stopping smoking will significantly reduce your risk of infection. If you are diabetic then having good control of your sugar levels will again significantly reduce your risk of developing an infection following surgery. Illnesses or medication which weakens the immune system such as diabetes, rheumatoid arthritis or immunosuppressant drugs increase the risk of infection as does obesity and smoking.
- Joint dislocation: If this occurs, the joint can usually be put back into place without an operation. Sometimes this is not possible, and an operation is required, followed by application of a hip brace. If your hip replacement remains unstable, further revision surgery may be required. The majority of dislocations occur in the first 12 weeks after surgery when the soft tissues are still healing so it is important you follow instructions from the nurses and physiotherapists.
Rare risks (occurs in less than 1% of those operated)
- Pulmonary Embolism (PE): a Pulmonary Embolism is the spread of a blood clot to the lungs and can affect your breathing. This can be fatal.
- Altered wound healing: the wound may become red, thickened and painful . Up to 40% of patients have difficulty lying on their hip after surgery.
- Nerve damage: efforts are made to prevent this; however there is a risk of damage to the small nerves of the hip. This may cause temporary or permanent altered sensation around the outside of the hip. There may also be damage to the sciatic nerve and this may cause temporary or permanent weakness or altered sensation of the lower leg. Occasionally this may require the use of an ankle brace.
- Bone damage: bone may be broken when the prosthesis (artificial joint) is inserted. This may require fixing either during the operation or at a later date.
- Death: This very rare complication may occur after any major operation. Overall the risk of dying after a hip replacement is very low, but death does occur in around 1 in 300 patients. The risk will be increased if you have medical problems such as heart or breathing problems and also increases with age. The risk of dying for someone aged over 80 for instance is over 1% and for those aged over 85 up to 3%.
Osteoarthritis of the hip exercises (MSK)
The exercises in the videos below have been provided to help with your hip pain. If there is any doubt about your fitness to do these exercises then please discuss this with your GP.
You may find that these exercises may slightly increase your symptoms initially. However you should find that the exercises themselves will become easier to do and that you begin to move your knee more easily. It can take around 12 weeks for you to notice a great improvement.
If the exercises do cause some discomfort, then taking prescribed medication from your GP or pharmacist may help you to continue to exercise.
If these exercises cause a large increase in your pain, or after 12 weeks there are no noticeable changes in your day to day symptoms, please contact your GP or NHS Inform for more advice.
The guide below will help ensure you are working at the right level.
Pain during exercise
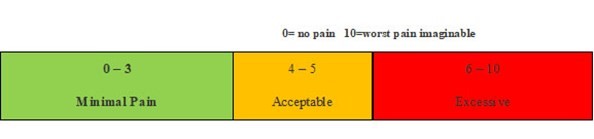
Within the scale, aim to stay in the green or amber boxes. If you are in the red area then you can modify the exercises by:
- reducing the amount of movement during an exercise
- reducing the number of repetitions
- reducing the weights
- reducing your speed
- increasing rest time between sets
Pain after exercise
Your pain or other symptoms should return to your pre-exercise baseline within 30 minutes of exercising. On the morning after your exercises, you should not feel an increase in pain or stiffness that lasts longer than 60 minutes.
Disclaimer
Please note: These exercises should not be used without prior consultation with a medical professional as the use of the wrong exercise may cause additional health related issues and discomfort. NHS Ayrshire & Arran and MSK NHS Ayrshire & Arran are not liable or responsible for any harm, losses or damages whatsoever resulting from the use or misuse of the information contained in or implied by the provided information in each video. These are provided for information only.
If you have any concerns about your ability to perform exercise then please discuss your concerns with your doctor or healthcare provider prior to participating in any advice that is on the MSK NHS Ayrshire & Arran website.
Please choose the most relevant exercise section for you.
Section 1: Mobility exercises
These exercises are designed to help improve your hip movements. Stop any exercise that significantly worsens your symptoms as per the pain chart above.
Exercise 1 – Pendulum Leg Swings
To do this exercise – stand side on a step with your painful leg hanging over the edge. You can use a banister or wall to assist with your balance. Gently swing the leg backwards and forwards like a pendulum.
Aim to swing 30 times, 3 times per day.
Exercise 2 – Supine Clam Stretch
To do this exercise – lie with your knees bent and feet hip width apart. Turn the soles of your feet to face each other and allow your knees to fall outwards. Feel the stretch in the groin. Keep your feet flat on the floor during the exercise. To increase the stretch add more pressure on the inner aspect of your knee and gently push towards the floor.
Hold for 30 seconds, repeat 5 times. 3 times per day.
Exercise 3 – Child’s Pose
To do this exercise – position yourself in the 4 point kneeling position.
Push your bottom back and down and the chest towards the floor. Let your arms slide along the floor as far as possible. Breathe out while doing the exercise.
Hold for 30 seconds, repeat 5 times.
Section 2: Strengthening exercises in a non-weightbearing position
Exercise 1 – Supine Buttock Squeeze
To do this exercise – lie on your back with both legs straight. Gently squeeze both buttock muscles together. Hold for 10 seconds and then release.
Aim to do 3 sets of 15 repetitions.
Exercise 2 – Prone Hip Extension (Knee Bend)
To do this exercise – lie on your stomach with both legs straight. Bend the knee of the painful leg to roughly 90 degrees. Squeeze both buttock muscles together. Slowly lift your foot towards the ceiling whilst lifting your thigh off the bed. Hold for 5 seconds and then slowly lower back towards the bed
Aim to do 3 sets of 15 repetitions.
Exercise 3 – Side-lying Hip Abduction
To do this exercise – lie on your non-painful side with the painful leg uppermost. Keep both legs straight. Lift the top leg towards the ceiling away from the other leg. Hold for 10 seconds and then slowly lower back towards the leg on the bed.
Aim to do 3 sets of 15 repetitions.
Exercise 4 – Prone Hip Extension
To do this exercise – lie on your stomach with both legs straight. Lift your painful leg towards the ceiling as far as you are able. Try and not over arch your lower back. Hold for 5 seconds and then slowly lower back to the starting position
Aim to do 3 sets of 15 repetitions.
Exercise 5 – Quadruped Leg Lift (Bird Dog)
To do this exercise – position yourself into the 4 point kneeling position. Then straighten your painful behind. Hold for 5 seconds and lower back to the starting position.
Aim to do 3 sets of 15 repetitions.
Section 3 – Strengthening exercises in a weightbearing position
Exercise 1 - Standing Hip Abduction
To do this exercise – rise into a standing position. Stand up straight and hold on to a chair with your painful leg on the outside. Use the chair to assist with your balance.
Slowly lift your painful leg out to the side as far as possible. Try to remain upright with your back straight. Hold the leg out as far as possible for 5 seconds and then slowly return to the starting position.
Aim to do 3 sets of 15 repetitions.
Exercise 2 – Standing Hip Extension
To do this exercise – rise into a standing position. Stand up straight and hold onto the back of a chair or wall to assist with your balance.
Keep the legs straight and slowly bring your painful leg backwards. Try to remain upright and do not bend your torso forwards doing this exercise. Hold the leg out as far as possible for 5 seconds and then slowly return to the starting position.
Aim to do 3 sets of 15 repetitions.
Exercise 3 – Bridging
To do this exercise – Lie on your back with knees bent and feet flat on the surface. Squeeze your buttocks together. Tilt pelvis backwards and then slowly lift you buttock muscles off the bed. Hold for 5 seconds and then slowly lower back to the starting position.
Aim to do 3 sets of 15 repetitions.
Exercise 4 – Chair Squat
To do this exercise – Rise into a standing position. Place your hands on both shoulders. Slowly lower your buttock back towards the chair. As soon as your bottom touches the seat slowly return to a standing position.
Aim to do 3 sets of 15 repetitions.
To make easier – use a higher chair or surface. To make a bit more challenging use a lower chair or step in your house.
Section 4 – Strengthening with a resistance band
Exercise 1 – Standing Hip Abduction (Resistance Band)
To do this exercise – rise into a standing position. Tie a resistance band round both ankles. Stand up straight and side on to a chair with your painful leg on the outside. Use the chair to assist with your balance.
Slowly lift your painful leg out to the side as far as possible. Hold the leg out as far as possible for 5 seconds and then slowly return to the starting position.
Aim to do 3 sets of 15 repetitions
Exercise 2 – Standing Hip Extension (Resistance Band)
To do this exercise – rise into a standing position. Tie a resistance band around both ankles. Use the chair to assist with your balance.
Keep the legs straight and slowly bring your painful leg backwards. Try to remain upright and do not bend your torso forwards doing this exercise. Hold the leg out as far as possible for 5 seconds and then slowly return to the starting position.
Aim to do 3 sets of 15 repetitions.
Exercise 3 – Side Lying Hip Abduction (Resistance Band)
To do this exercise – lie on your non-painful side with the painful leg uppermost. Tie a resistance band round both ankles. Lift the top leg towards the ceiling away from the other leg. Hold for 10 seconds and then slowly lower back towards the leg on the bed.
Aim to do 3 sets of 15 repetitions.